If you are a teacher of movement classes that are safe for people with osteoporosis please contact us and provide us with the details of your class: Class Name, Teacher Name, Street Address, City, State, Dates and Times! We are collecting a database of safe movement classes for people to find a teacher in the Bay Area and across the USA. Click here to email details to us...
We have a new Video Library available with new Bone-Safe and Bone-Building Pilates Mat Classes uploaded every week! All of our DVD workouts are now available in the Online Video Library.
Click the link above to download the handout from the Fletcher Pilates Conference "Research Update on Exercise for Osteoporosis lecture by Dr. Sherri Betz. References are also included in the handout after the slides.
Read the many updates on exercise for kyphosis, vertebral fracture and hip fracture from Kathy Shipp, PhD, PT, and Wendy Katzman, PT, DSc, OCS, researcher at UCSF, Exercise for Osteoporosis Research by Debbie Rose, PhD, and Karen Kemmis, DPT. Also read controversial reviews on the relationship Calcium to Cardiovascular Events by Dr. Andrea Singer and much more...
Published in the April 2005 edition of the IDEA Fitness Journal. This article is a comprehensive look at the Pilates for Osteoporosis Program here at TheraPilates.
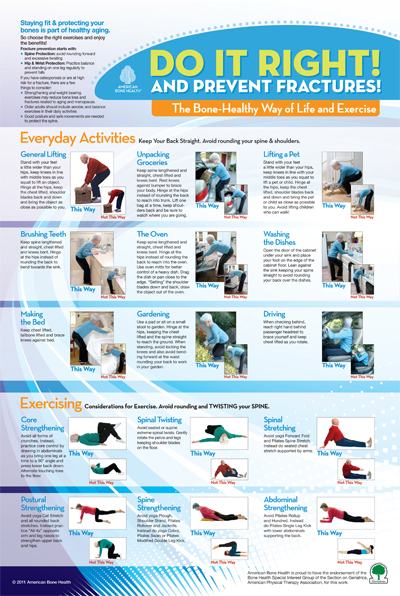
89% of the participants in this study suffered an additional compression fracture after participating in flexion (curl up) exercises. Gives the scientific support and rationale for avoiding all spinal flexion exercises in those with low bone density!
Dr. Tom McGuire, holistic dentist and researcher, who has focused his practice on education of the perils of mercury fillings, wrote a wonderful and comprehensive paper filled with resources and recommendations for nutrition, supplementation, medication and exercise for osteoporosis that he discovered through helping his wife deal with the diagnosis and repercussions of osteoporosis. There are some very interesting findings on the benefits of supplementing with Vitamin K2 (Especially MK-4 and MK-7) that have shown promising findings in a few studies. Get all the details in this comprehensive paper!
Podcasts and Articles written by Sherri Betz, PT, GCS, Available on Other Web Sites
An ADVANCE interview with geriatrics specialist Sherri Betz, PT.
from Advance Magazine for Physical Therapists, Oct. 2004
Frequently asked questions about Pilates and Osteoporosis
QUESTION #1: Why can't a person with Osteopenia flex the spine?
Regarding the difference between osteoporosis and osteopenia: Basically we must assume that if the person has osteopenia of the lumbar spine that they may very likely have osteoporosis of the thoracic spine. 1)The thoracic spine is more oriented to kyphosis and anterior loading of the vertebral bodies, 2)The vertebrae get smaller as we go up the vertebral column and 3) The most popular fracture site of the spine is at T6-T7 and T8. We also have no way of determining whether or not the disease is progressing as we are working with our clients. There is no way we can determine how much force it would take to cause a fracture in the spine. The statistics are clear; 1 in every 2 women over age 50 will have an osteoporotic fracture in their lifetime. Then after the 1st vertebral fracture the risk of having another one within 1 year is 500%!! We need to be very vigilant about preventing the 1st fracture. It's not a good idea to “experiment” with clients when the research is very clear. A physical therapist is guilty of malpractice if they put a patient who has known osteoporosis in spine flexion.(Carole Lewis, PT) I am in support of “evidence-based” practice in PT and Fitness. I want to give my clients/patients SAFE exercises that WORK! Unfortunately with so many flexion exercises in our beloved Pilates method we are forced to be creative and compliant. Yes, we WILL narrow their options for movement somewhat but my clients from age 20-84 are completely happy with their exercise programs and feel very confident about their guidelines and exercises! They don’t want to have any/anymore fractures! I know very few people on the planet these days that need to increase their degree of thoracic flexion!
There is an article that explains all of the reasons for avoiding flexion, Modifying Pilates for Osteoporosis, published April 2005 in the IDEA Fitness Journal. It is downloadable on this webpage: http://www.therapilates.com/osteonews.html
QUESTION #2: My understanding is that if a person has osteopenia, they are to be treated as though they have osteoporosis (no flexion, rotation, and side bending)?
Yes, we do not know how the disease is progressing as we are working with the client. We also don’t know exactly what the BMD is of the thoracic spine (BMD testing is done on the lumbar spine…) We must teach the client how to avoid flexion, sidebending and rotational loads on the spine with a special focus on protecting the thoracic spine (the most popular site for fractures is T6-7-8). Rotation causes significant loading and compression of the vertebral bodies and is greatest in upright postures. Review the study on partial curlups by Sinaki in 1984, that showed that 89% of the people in the study who performed partial curlups had an additional fracture! This 4 page study is downloadable on this webpage at http://www.therapilates.com/osteonews.html
.
Sinaki M, Mikkelsen, BA “Postmenopausal spinal osteoporosis: Flexion versus extension eexercises.” Arch Phys Med Rehab 1984; 65; 593-596.
QUESTION 3: If a person has osteopenia or osteoporosis only in the hip and has normal bone mineral density in the lumbar spine, do we have these same contraindications for avoiding spinal flexion, rotattion and sidebending?
No, we can be a little bit more liberal with movements of the spine. For instance, if it is the clients 1st BMD, we don’t know the trend in bone loss. If we have seen improvements in several BMD Reports we can assume that BMD is either stabilized or increasing. Also, we must understand that osteoporosis is a "systemic" condition. We don't know if the bone loss will eventually affect the vertebral bodies. We must consider the clients spinal shape. Do they have an ideal postural alignment or do they have an increased thoracic kyphosis? If an increased thoracic kyphosis is present then we would certainly need to avoid thoracic flexion exercises. I still don't advocate extreme loading of the spine at endranges of spine flexion, sidebending or rotation if low bone density has shown up in any body part. Again, our first priority is to prevent the first fracture!
QUESTION #4: If someone has an increased thoracic kyphosis or a dowager's hump does that mean that they have osteoporosis?
Bones remodel their shape in response to the forces placed upon them. So, if someone sits regularly in slumped posture, their vertebral bodies or spinal bones might reshape into wedge shapes without the presence of osteoporosis.
QUESTION #5: What are the contraindications for hip osteoporosis?
Extreme external or internal rotation of the hip as in the mermaid exercise position of the legs especially in someone who has "tight" hips or a tight capsule. The client who can't sit comfortably in the Mermaid or a cross-legged position should avoid sitting in that position all together. Also, the "Pigeon" pose in Yoga should be avoided. Another cause of low bone density hip fracture is turning on a planted foot. Clients should be educated about turning their feet with the body when they change directions in standing.
QUESTION #6: What about clients who have osteopenia or osteoporosis who want to play golf?
Many clients with osteoporosis and osteopenia are golfers. It depends on the degree of bone loss, and the client must be advised of the risks. Golf swings can begin in neutral spine, and the swing ends in Spinal Extension and Rotation which is not contra-indicated. They just need to learn spine awareness and to avoid flexion at the beginning of their swing and avoid extreme sidebending at the end of the swing (coach them to stay elongated as they finish their swing.) Extension intuitively feels like bone on bone at end range. The posterior part of the vertebrae (pars intra-articularis) is mostly made up of cortical bone and is stronger and very fracture resistant. The client often reports that they avoid extension exercises because "they feel like the spine is going to break." This client must be educated that this extension movement is permitted and desirable and actually helps to build bone mineral density and prevent vertebral fractures.
Sinaki M, McPhee MC, Hodgson SF, Merritt JM, Offord KP. "Relationship between bone mineral density of spine and strength of back extensors in healthy postmenopausal women." Mayo Clin Proc. 1986 Feb;61(2):116-22.
Sinaki M, Wollan PC, Scott RW, Gelczer RK. "Can strong back extensors prevent vertebral fractures in women with osteoporosis?" Mayo Clin Proc. 1996 Oct;71(10):951-6.
Salads Save Bones!
A July 2002 Swiss university study has confirmed earlier research showing that onions, herbs, such as parsley, garlic and dill, and common salad vegetables, such as lettuce, arrugula, cucumber and tomato, improve bone metabolism and reduce bone loss.
In the initial research, rats given common herbs and vegetables, such as onion, parsley and salad greens, were found to have significantly less bone loss compared to rats not on the vegetable-enriched diet. Onion, in particular, was found to not only inhibit bone resorption, but to actually increase bone mass.
Surprisingly, powdered cow’s milk, a food often touted as effective in helping to prevent osteoporosis, had no effect on the rate at which the rats' bone was broken down and reabsorbed.
Researchers have speculated that vegetables help prevent bone loss by promoting a more alkalkine pH in the body, but this most recent research suggests that onions and other vegetables and herbs exert beneficial effects on bone that are not limited to their buffering of an acid pH in the body, which is thought to dissolve bone.
Sherri's Osteogenic Salad Recipe!!
Trader Joe's Items:
Arugula
Carrot Sticks
Broccoli
Cucumbers
White Mushrooms
Cherry Tomatoes
Parmesan or Romano Grated Cheese
Toasted Sesame Oil
Tamari Roasted Almonds
Traditional Grocery Store Items:
Fresh Dill
Fresh Parsley
Canned Chickpeas
Canned Beets
Marukan Rice Wine Vinegar (Yellow Label)
Toss all items, sprinkle with Sesame Oil and Rice Wine Vinegar and enjoy!
More Practical Tips:
Here are a few of the World’s Healthiest Foods quick serving ideas to help you reap the bone-saving benefits of these vegetables and herbs.
•
Add sautéed chopped onions to soups or most any vegetable dish
•
Place small boiling onions on a skewer, either alone or with other vegetables, coat lightly with olive oil and grill for approximately ten minutes.
•
Combine dill, plain yogurt, chopped onion and chopped cucumber for a delicious cooling dip
•
Add dill and chopped onion to your favorite salad recipe.
Research Summary:
In the initial research, rats given common herbs and vegetables, such as onion, parsley and salad greens, were found to have significantly less bone loss compared to rats not on the vegetable-enriched diet.
Small amounts of several vegetables and vegetable mixtures produced a significant drop in the rate of bone loss—just 500 mg daily each of onion and Italian parsley, and 100 mg each of a mixture of lettuce, tomato, cucumber, arrugula, onion, garlic, wild garlic, common parsley, Italian parsley, and dill had protective effects on bone mass. Not only did the rats’ consumption of these vegetables and herbs inhibit bone resorption, but onion was actually shown to increase bone mass.
Researchers were surprised to find that powdered cow’s milk, which has long been thought to be effective in helping to prevent osteoporosis, had no effect on the rate at which the rats' bone was broken down and reabsorbed.
Researchers have speculated that vegetables help prevent bone loss by promoting a more alkalkine pH in the body, but this most recent research suggests that onions and other vegetables and herbs exert beneficial effects on bone that are not due to their buffering effect on metabolic acid, which is thought to dissolve bone.
In the July 2002 study, Swiss researchers showed that, although the rats' intake of onion was associated with a decrease in urinary acid excretion and a concomitant inhibition of bone resorption, other experiments showed that the two findings were not causally related. In these experiments, onion was shown to increase the inhibition of bone resorption even when it was given in addition to an already aklaline vegetarian diet. And onion and a mixture of vegetables, salads, and herbs were found to increase the inhibition of bone resorption even when metabolic acid was already buffered by potassium citrate. In addition, neither the pH nor the potassium content of the individual vegetables, salads, and herbs reaches a level that would inhibit bone resorption if this effect were due primarily to the production of a more alkaline pH.
Since the research shows that the protective effects on bone produced by vegetables, salads, and herbs are not merely due to their metabolic alkalinity, scientists are now theorizing that the bone-boosting effects are due to pharmacologically active compound(s) in the herbs and vegetables. Future research will undoubtedly uncover the compounds responsible, but fortunately, we don't have to wait to reap the bone-saving benefits. All we need to do is enjoy lots of onions, garlic, parsley, dill, tomatoes, cucumbers and green leafy salads.
References:
Muhlbauer RC, Li F. Effect of vegetables on bone metabolism. Nature 1999 Sep 23;401(6751):343-4.
Muhlbauer RC, Lozano A, Reinli A. Onion and a mixture of vegetables, salads, and herbs affect bone resorption in the rat by a mechanism independent of their base excess. J Bone Miner Res 2002 Jul;17(7):1230-6
Osteoporosis: Can you prevent it?
Osteoporosis has become a national epidemic. Osteoporosis is the gradual and silent loss of bone, which is primarily affecting post-menopausal Caucasian women. In my practice as a physical therapist I have found that the patients I work with are younger and younger. I used to only treat patients with osteoporosis in nursing homes and now Im beginning to see osteoporosis more frequently in outpatient facilities. It has been reported that 20 million Americans are affected by osteoporosis and this number is expected to rise to 53 million by the year 2030. What are we doing wrong? In my opinion, the American lifestyle is the culprit. We base our habits of daily living on convenience and time management. We have computers for shopping, TV to entertain us, washing machines, elevators, escalators, cars and high tech devices to save time and to make our lives more efficient. These high tech efficiencies are killing us!
What can we do to help ourselves? Nutrition, Environment, Healthy Relationships and Exercise are all part of a balanced lifestyle in which all of the components must be included to stay well, build bone and prevent as well as reverse osteoporosis. It has been shown that exercise alone can halt the progression of osteoporosis in most cases. As much as 20% of bone can be built in one year through modifications in nutrition and bone building exercises such as spinal stabilization and Pilates-Based Exercise (yes, Pilates is a form of bone building exercise).
Osteoporosis most commonly affects the spinal vertebrae, hips and wrists. Post-menopausal women have a greater susceptibility to bone loss due to the decrease of estrogen and progesterone. Estrogen stimulates bone growth while progesterone inhibits bone loss. This is the reason many women are placed on HRT-hormone replacement therapy (combination of estrogen and progesterone) after menopause. The risks of hormone replacement therapy are well known and many women are opting to go the natural route through lifestyle modification, nutritional changes and exercise. My goal as a physical therapist is to dispel the myth that aging means decline and that arthritis and osteoporosis are not a natural part of aging.
Bone Densitomitry is recommended (by us, not everyone) at age 40 for a baseline bone density. DEXA (Dual Photon Xray Absorptiometry) is the method usually used to determine bone density. If you have results that are positive for low bone density (Osteopenia) or full Osteoporosis it is recommended that you make the necessary changes suggested by your health care professional. Have a Bone Density Study repeated every 2 years to see if you are on the right track with your treatment or prevention program.
If you have any questions regarding Osteoporosis, please:
call 318-450-1747 or email Sherri Betz, PT at TheraPilates® Physical Therapy for a phone consultation.